
Reporting lesions in the bowel cancer screening programme.
Guidelines from the bowel cancer screening programme
pathology advisory panel.
- Professor Frank Carey (Dundee)
- Dr Mark Newbold (Coventry)
- Professor Phil Quirke (Leeds - Chair)
- Professor Neil Shepherd (Gloucester)
- Dr Bryan Warren (Oxford)
- Professor Geraint Williams (Cardiff)
Dissection of submitted lesions
Key diagnostic features to be discussed
Introduction
The NHS bowel cancer screening programme will in due course become the largest programme for bowel cancer screening in the world. It offers a unique opportunity to improve survival in this condition as well as clarifying the importance of current diagnostic criteria and identifying the biological potential of precursors of colorectal cancer.
These guidelines are produced under the auspices of the NHS bowel cancer screening programme. They have been derived to answer many of the questions that have arisen within the pilot centres, to ensure that key data is collected in a consistent manner and to enable further recommendations to be made to provide the best possible evidence base for routine practice.We welcome feedback and will develop these guidelines as the evidence base improves in the future. We are striving to ensure consistency across the four devolved UK Nations and between the published recommendations of concerned professional organisations such as the Royal College of Pathologists, British Society of Gastroenterology and the Association of Coloproctology of Great Britain and Ireland. We have also built on the pathology work undertaken during the CRUK flexisigmoidoscopy trial by adopting many of the definitions we developed for that trial. These guidelines are consistent with the Royal College of Pathologists Dataset for reporting colorectal cancer (including local excision specimens) and will be developed closely with them in the future.
General issues
Dysplasia is divided into low and high grade to improve interobserver agreement, with 'high grade dysplasia' equating to 'severe dysplasia' in older systems(1). The term hyperplastic rather than metaplastic polyp is recommended. Neither is a good name but adding a third only confuses matters further. The reasons are that firstly, the term hyperplastic has been used in both pilot centres; secondly, true metaplasia (e.g. squamous islands) can rarely occur in dysplastic adenomas and thirdly, the term metaplastic is defined as a change in epithelial type from one mature epithelial type to another. Whilst the epithelium of a hyperplastic lesion is abnormal it is not of a different epithelial type. Different antigenic patterns have been demonstrated in hyperplastic polyps but these are not those of another mature epithelial type. Polyps have been broadly sub-classified into classical type, hyperplastic-serrated spectrum and other types of lesion. We have concentrated on early invasive lesions as these have proved challenging within the pilot centres, the evidence base is currently poor and the screening programme will generate many of these difficult lesions. We have also sought to identify the serrated spectrum to allow further investigation in this area.
Pathologists must complete either the screening programme proforma or the computerised version of the form to be returned to the screening coordinator. They may in addition wish to also provide a free text report directly to the clinician.
Dissection of submitted lesions
The material received will be either a biopsy of a lesion, an excision of a polyp or a submucosal resection of a sessile lesion or a larger resection either a trans-endoscopic mucosal excision (TEM) or a full surgical excision.
Where only a biopsy is received then the size of the lesion and completeness of excision will not be assessable by the pathologist and these should be recorded as n/a.
While the principles of pathological reporting are the same as in major resections, a number of features require special attention in local excisions of (presumed) early cancers with curative intent because they are used to determine the necessity for more radical surgery. In addition to the assessment of completeness of excision, these include the recording of parameters that predict the presence of lymph node metastasis in early tumours, namely tumour size, poor differentiation, the depth of invasion into the submucosa and the presence of submucosal lymphovascular invasion.(2-7) However, there is only limited evidence and no consensus in the published literature on how exactly some these parameters should be assessed or how they, especially the depth of submucosal invasion should be assessed. We hope to improve this situation from data derived from the screening programme.
Local excisions are undertaken endoscopically or, in the case of early rectal tumours, under direct vision. The majority of carcinomas arise within pre-existing adenomas that may be polypoid, sessile or flat, and the best pathological information is derived when lesions are excised in their entirety to include both the invasive and preinvasive components.(8) Polypoid lesions on a narrow stalk can be fixed intact, while sessile lesions should be pinned out, mucosal surface upwards, on a small piece of cork or other suitable material, taking pains to identify the narrow rim of surrounding normal tissue, before fixing intact. Piecemeal removal of tumours, entirely acceptable for palliative resections, should be avoided because it precludes a reliable assessment of completeness of excision.
After fixation, polypoid lesions may be bisected through the stalk if they measure <10mm; larger polyps are trimmed to leave a central section containing the intact stalk, and all fragments embedded for histology. It is recommended that at least three sections are taken from blocks containing the stalk. The margins of larger, sessile lesions should be identified with appropriate coloured markers (inks or gelatine) and the whole of the specimen transversely sectioned into 3 mm slices and submitted for histology in sequentially labelled cassettes. In cases where the margin of normal tissue is less than 3 mm, a 10 mm slice containing the relevant margin should be made and further sectioned at right angles.
Key diagnostic features to be discussed:
Site
The site of origin of each specimen should be individually identified by the clinician and provided to the pathologist on the request form. The pathologist should record this on their proforma. This is important information as the risk of lymph node metastases from a T1 adenocarcinoma varies depending on the site of the lesion.(7)
Type
Three broad groups of lesion are reported, namely classical adenomas, serrated lesions, and other polyps. Classical adenomas are divided into tubular, tubulovillous or villous types. The spectrum of lesions with a serrated growth pattern is subdivided into hyperplastic polyps, mixed dysplastic/hyperplastic adenomas and serrated adenomas. Other types of polyp include inflammatory polyps, juvenile polyps, Peutz-Jeghers or other types which are included under not otherwise specified and described in free text.
Classical adenomas
By definition, adenomas must show dysplasia. They can be of tubular, tubulo-villous or villous types and demarcation between the three is based on the relative proportions of tubular and villous components, according to the '20% rule' described in the WHO classification.(8) At least 20% of the estimated volume of an adenoma should be villous to classify a polyp as tubulovillous and 80% villous to be defined as a villous adenoma. All other lesions are classed as tubular.
The 20% rule only applies to wholly excised polyps and to intact sections of lesions large enough to provide reliable proportions. For small fragmented lesions or superficial polyp biopsies, the presence of at least one clearly identifiable villus merits classification as "at least tubulovillous".
Villousness
While it is accepted that a neoplastic villus almost defies definition, the following descriptions have been developed to help recognize 'villousness'.
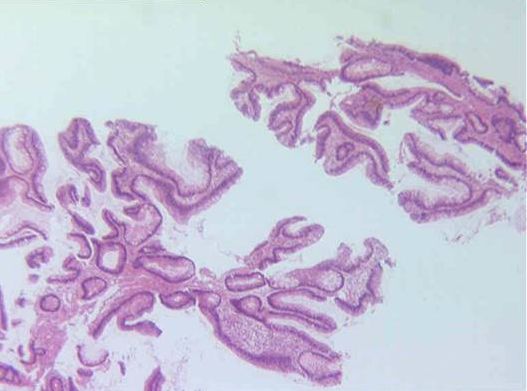
Figure 1. A fragmented biopsy showing a villous component
Villous structures may take different forms that in themselves are not known to have any particular significance but may assist observer reproducibility. These include:
- "Classical" villi composed of long, slender, upgrowths of epithelium on a thin delicate stromal core that branches little. These usually have parallel sides (though sometimes a bulbous tip), and often appear to extend right down to the muscularis mucosae.
- "Palmate" villi composed of clustered, broader, branching, leaf-like structures with a hand-like configuration. Tubular glands may be present at the base of these structures and sometimes may even be present within the stromal core of villi.
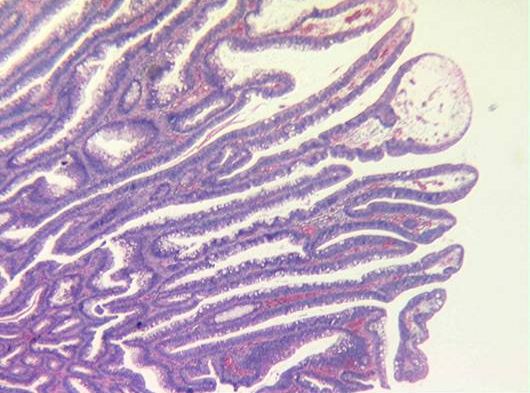
Figure 2. An example of classical villi which should provide little difficulty to a pathologist. The bulbous tip that can be seen is well demonstrated
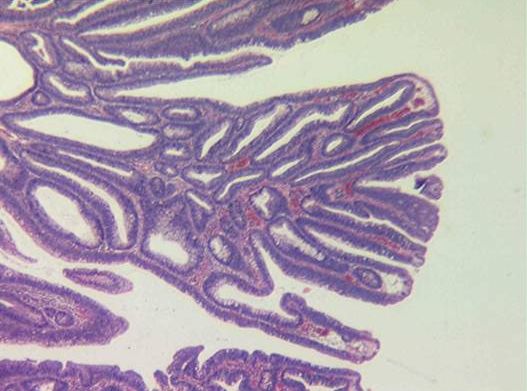
Figure 3 Example of palmate villi
- "Foreshortened" villi composed of slender non-branching outgrowths with a thin stromal core that clearly protrude beyond the overall surface contour of an otherwise well developed tubular lesion.
Most diagnostic difficulties will arise with foreshortened villi, particularly in distinguishing "true" villi from exaggerated, axially sectioned, neoplastic crypts with distended luminal openings. In these situations, it is better to err on the side of under-diagnosis of villous change, especially in small (<1 cm) adenomas, and to restrict the term to lesions where there are convincing outgrowths.
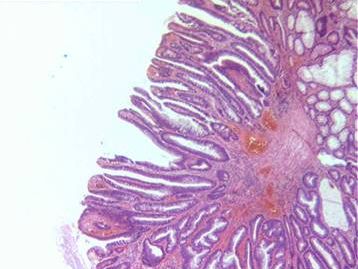
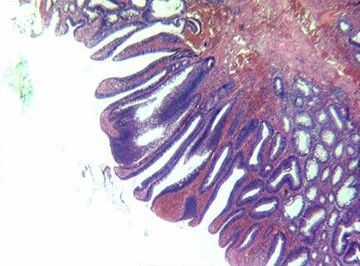
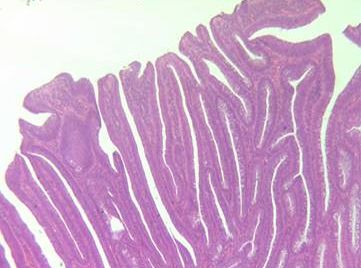
Figure 4. Examples of tubulovillous adenomas.
Villous structures with low grade dysplasia not infrequently show a characteristic quality to the epithelium, with rows of regular tall columnar cells with large conspicuous apical mucin vacuoles that are reminiscent of the surface epithelium of the stomach. This is in contrast to the typical goblet cells interspersed with eosinophilic colonocytes containing sparse or no obvious mucin which are characteristic of tubular adenomas. The presence of such a "mucinous" epithelium should sway the diagnosis in favour of villous histology if it is conspicuous in an otherwise indeterminate lesion.
Hyperplastic - Serrated adenoma spectrum
The pathology of serrated lesions is currently an active area of research and there is a limited evidence base for the relative importance of some of the phenotypes that have been described in the literature(9). In the light of this the current guidelines identify practical categories that may be studied further and sub-categorised in future when more evidence is available. In the spectrum are non dysplastic hyperplastic polyps, dysplastic lesions with a serrated architecture called here serrated adenomas, and mixed hyperplastic/adenomatous polyps.
Hyperplastic Polyps
The architecture of the glands can vary from normal to grossly distorted. Usually demonstrate elongated crypts with an excess of columnar absorptive cells leading to a tufted, crenated appearance towards the surface. A variable degree of epithelial proliferation can be seen in the base of the crypts. The cells are cytologically regular with no dysplasia present.
Serrated adenomas
These lesions have the morphology of hyperplastic polyps, namely a serrated epithelial surface with plentiful eosinophilic cytoplasm but they show definite dysplasia throughout the lesion.
For example:
Serrated adenoma example
Mixed hyperplastic/adenomatous polyps
These lesions have both non dysplastic hyperplastic-type epithelium showing a serrated glandular architecture and areas of adenomatous dysplastic epithelium. The two phenotypes are morphologically distinct, and although they may intermingle, individual glandular structures showing both patterns are not present.
For example:
Mixed hyperplastic/adenomatous polyp example
Other types
Inflammatory polyps
Experience from NHSBCSP pilot sites has shown that inflammatory-type polyps are relatively common. Whilst they are most usually seen as a complication of chronic inflammatory bowel disease, particularly ulcerative colitis, they are also seen in association with diverticulosis, mucosal prolapse and at the site of ureterosigmoidostomy. Furthermore, sporadic single inflammatory-type polyps are well described in the colorectum. As the reporting pathologist may not know the true context of such polyps, we recommend that all such polyps are classified as "inflammatory polyp".
Juvenile polyps
Classical juvenile polyps are spherical in shape, show an excess of lamina propria and have cystically dilated glands. The expanded lamina propria shows oedema and mixed inflammatory cells. Experience from the NHSBCSP pilot sites suggests that occasional juvenile-type polyps are identified, even in the screening age group. Juvenile polyps are, of course, most common in children but occasional examples are seen in adults. It remains uncertain whether the juvenile-type polyps identified in the screening population are true classical juvenile polyps or whether they represent inflammatory-type polyps with mimicry of classical juvenile polyps. We advise that any polyp showing juvenile polyp-type features should be classified as "Juvenile polyp" for the purposes of diagnostic reporting in the NHSBCSP. In classical juvenile polyps, there is often epithelial hyperplasia but dysplasia is very rare with a handful of case reports in the literature(10).
So-called "atypical juvenile polyps" show different morphological features, with a multilobated architecture, intact surface mucosa (usually) a much more pronounced epithelial component. They are a characteristic feature of juvenile polyposis (JP). It would seem most unlikely, given the rarity of JP and the age of the screening population, that such polyps might be seen in the NHSBCSP. Such a polyp should be recorded as representing "juvenile polyp". They are much more likely to harbour epithelial dysplasia(11).
Peutz-Jeghers polyps
Whilst these polyps are usually seen in the Peutz-Jeghers syndrome, occasional examples are demonstrated as single sporadic polyps in the colon. There remains uncertainty as to whether "inflammatory myoglandular polyp" represents a similar entity. As with juvenile polyposis, it would seem most unlikely, given the rarity of the syndrome and the age of the screening population, that Peutz-Jeghers syndrome would be diagnosed as part of the NHSBCSP. Although Peutz-Jeghers polyps are classified as hamartomas, they have a very organised structure. They have a central core of smooth muscle with conspicuous branching, each branch being covered by colorectal-type mucosa which appears hyperplastic but not dysplastic. As with sporadic juvenile polyps, solitary Peutz-Jeghers-type polyps are most unlikely to demonstrate foci of dysplasia.
Cronkhite-Canada syndrome
We believe it is most unlikely that such cases will present via the NHSBCSP and the true diagnosis may not be recognised by pathological assessment. Such polyps are probably best regarded as of inflammatory type.
Other polyps, including carcinoids and stromal polyps
Small rectal mucosal nodules, showing the characteristic features of hind gut carcinoids, are not uncommon. For pathological reporting as part of the NHSBCSP, we recommend that these are recorded as "other polyp" and their true nature recorded in free text. Furthermore, there are a number of stromal tumours which can also present as polyps. Lipoma and leiomyoma of the muscularis mucosae are probably the most likely to be seen in the NHSBCSP and we recommend that these are recorded as "other polyp" and their true nature recorded in free text. North American experience with bowel cancer screening indicates that, rarely, other unusual forms of stromal tumour can present as polypoid nodules in the screening programme. Such stromal lesions include ganglioneuroma, neurofibroma, GIST, various forms of vascular tumour, perineurioma, fibroblastic polyp and epithelioid nerve sheath tumour.
Shape
The NHS bowel cancer screening programme is not designed to detect flat adenomas as it does not mandate magnifying endoscopy or chromoendoscopy. They have not been separately identified at this stage but this area will be revisited in the future in the light of experience. The current pilots only see these lesions rarely in their material.
Size
An accurate measurement is very important and measurement must be to the nearest mm (and not 'rounded-up' to the nearest 5 or 10mm). This will be audited. The maximum size of the lesion should be measured from the formalin fixed macroscopic specimen where possible. For small lesion(s), 5mm or less, that fit on one section in their entirety it is acceptable to measure its dimensions from the glass slide. If a biopsy is received then n/a should be entered in the size box.
Dysplasia
We recommend that high grade dysplasia and low grade dysplasia are used instead of mild, moderate and severe dysplasia. This will increase the interobserver agreement and allow pathologists to concentrate on the important diagnostic criteria.
High grade dysplasia
The changes of high grade dysplasia should usually involve more than just one or two glands (except in tiny biopsies of polyps), sufficient to be identified at low power examination. Caution should be exercised in over interpreting isolated surface changes that may be due to trauma, erosion or prolapse.
High grade dysplasia is diagnosed on architecture, supplemented by an appropriate cytology. Hence its presence is nearly always suspected by the low-power appearances where complex architectural abnormalities are present in structures whose epithelium looks thick, blue, disorganised and "dirty". The architectural features are:
- complex glandular crowding and irregularity (Note that the word "complex" is important and excludes simple crowding of regular tubules that might result from crushing)
- prominent budding (Note that the word "prominent" is important; there is probably some degree of glandular budding, by definition, in all tubular adenomas)
- a cribriform appearance and "back to back" glands
- prominent intraluminal papillary tufting
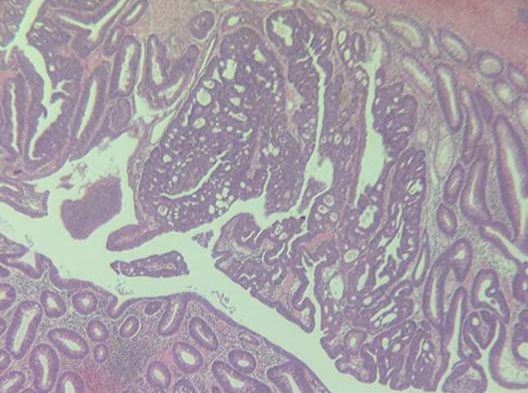
Figure 5A) High grade dysplasia showing architectural changes
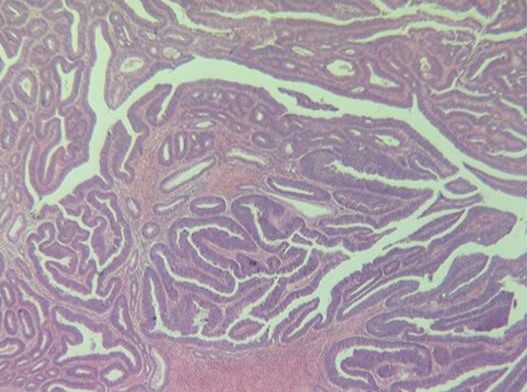
Figure 5B) Another area of high grade dysplasia from the same case showing a lesser degree of architectural abnormalities.
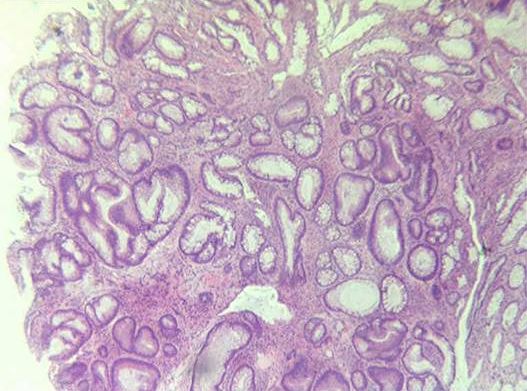
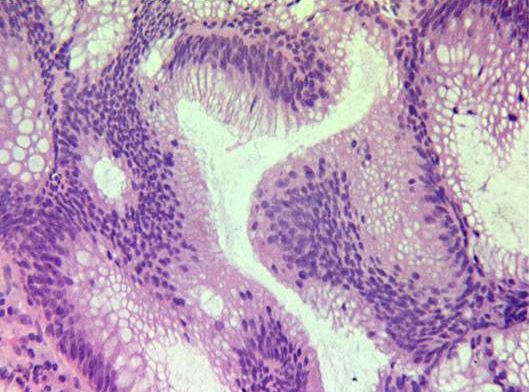
Figure 6. A) and B)
The changes shown here are not those of high grade but of low grade dysplasia because of the architectural changes. The cytology is less worrying.
While many of these features often coexist in high grade dysplasia, individually they are neither necessary nor usually sufficient. Indeed they may occasionally occur in lower grades of dysplasia, which is why it is necessary to go on to scrutinise the cytological features for signs of high grade dysplasia. These are:
- loss of cell polarity or nuclear stratification to the extent that the nuclei are approximately equally though haphazardly distributed within all three thirds of the height of the epithelium
- markedly enlarged nuclei, often with a dispersed chromatin pattern and a prominent nucleolus
- atypical mitotic figures
- prominent apoptosis, giving the lesional epithelium a "dirty" appearance.
Again, these features usually coexist in high grade dysplasia, and caution must be exercised in using just one. It should be emphasised again that they should occur in a background of complex architectural abnormality. Marked loss of polarity and nuclear stratification sometimes occurs on the surface of small, architecturally regular, tubular adenomas that otherwise have a lower grade of dysplasia, probably as a result of trauma, and must not be used to classify a lesion as high grade. The only exception to the rule is when the specimen consists of just a small biopsy from a polyp, when there is insufficient tissue to assess the architecture properly. In this situation it is permissible to label florid cytological abnormalities alone as high grade dysplasia, but this will usually lead to re-excision of the whole polyp, when it will be possible to assess the whole lesion properly.
ADENOCARCINOMA
Definition of invasion
We recommend the use of the definition of an adenocarcinoma that is in everyday use within the United Kingdom of invasion of neoplastic cells through the muscularis mucosae into the submucosa of the bowel wall.
This definition disallows the diagnosis of intramucosal carcinoma and such cases should be considered high grade dysplasia. We recognise that this will not allow comparison with Japanese series where a diagnosis of carcinoma can be made on cases of high grade dysplasia without invasion but is compatible with the USA and European literature.
Epithelial misplacement:
Epithelial misplacement of adenomatous epithelium into the submucosa of a polyp is a well recognised phenomenon(12). It is commonly seen in prolapsing polyps in the sigmoid colon. Experience from the pilots suggests that this will be one of the most difficult areas of pathological diagnostic practice in the NHSBCSP. These sigmoid colonic polyps are particularly prone to inflammation and ulceration, features which tend to enhance the dysplastic changes present. When associated with epithelial misplacement, the potential for misdiagnosis of early carcinoma and the overall diagnostic difficulties become much greater. We propose that the provision of an expert group, perhaps the NHSBCSP Pathology Committee members, can aid in the pathological assessment of such cases, although this requires ratification at the current time.
For an example of epithelial misplacement:
Epithelial misplacement example
Early adenocarcinomas (pT1)
Tumours that invade the muscularis propria (pT2) usually require further surgery and should be staged according to the cancer minimum dataset.
pT1 tumours will provide many difficulties in the programme and the current evidence base for its management is poor thus as a priority we have chosen to concentrate on generating a firm evidence base for management. This will require a limited number of extra assessments that we will then refine on the basis of the data emerging from the pilots and the programme. In particular sub-staging and differentiation grading are addressed.
Sub-staging
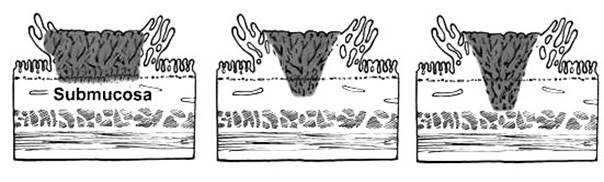
In pT1 tumours the frequency of lymph node metastasis in sessile tumours that involve the superficial, middle, and deep thirds of the submucosa (so-called Kikuchi levels sm1, sm2 and sm3 respectively(6)) has been reported to be 2%, 8% and 23%.(7)
 | ||||
|---|---|---|---|---|
Figure 7a Kikuchi levels of submucosal infiltration (from Nascimbeni et al(7))
In polypoid lesions, Haggitt et al(5) identified the level of invasion into the stalk of the polyp as being important in predicting outcome and found that 'level 4' invasion, in which tumour extended beyond the stalk of the polyp into the submucosa but did not invade the muscularis propria, was an adverse factor.
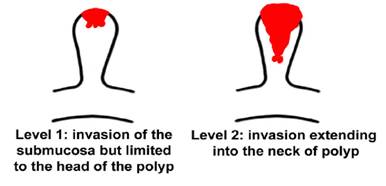
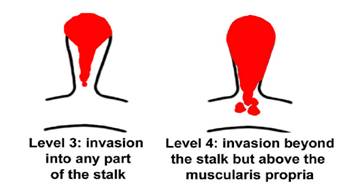
Figure 7b Haggitt levels of invasion in polypoid carcinomas
However, neither Kikuchi (for sessile tumours) nor Haggitt (for polypoid tumours) systems are always easy to use in practice, especially if there is fragmentation or suboptimal orientation of the tissue, and one study found lymph node metastases in 6/24 Haggitt level 3 lesions(5). More recently Ueno et al(13) have proposed that the depth of invasion measured in microns beyond the muscularis mucosae provides a more objective measure and has been adopted in Japan. Each classification has advantages and disadvantages. Kikuchi cannot be used if there is no muscularis propria, Haggitt is of no value in sessile lesions and measurement depends on a recognisable submucosa from which to measure from. In view of the uncertainty and lack of consensus, a firm recommendation for one method of assessing local invasion cannot be made, and all three approaches are included on the template proforma to be filled in so that a future analysis can compare the value of these sub-staging methods.
Tumour grade
Poorly differentiated carcinomas are identified by the presence of either irregularly folded, distorted and often small tubules or the lack of any tubular formation. In the absence of good evidence we recommend that a grade of poor differentiation should be applied in a polyp cancer when ANY area of the lesion is considered to show poor differentiation. This differs from that recommended for major colorectal cancer resections in the RCPath Dataset where grade is determined on the predominant area. Applying the 'worst area' criterion will allow all potentially poorly differentiated tumours to be identified for research into which of the two approaches is better for identifying T1 cancers at increased risk of lymph node metastases for major resection without exposing such patients to the possibility of under treatment. An early review of poorly differentiated pT1 cases will be undertaken.
Lymphovascular invasion
Definite invasion of endothelium-lined vascular spaces in the submucosa is generally regarded as a significant risk for lymph node or distant metastasis. Sometimes retraction artefact around tumour aggregates can make assessment uncertain, in which case this uncertainty should be recorded and the observation interpreted by the MDT in the light of any other adverse histological features.
Margin involvement
It is important to record whether the deep (intramural) resection margin is involved by invasive tumour (which may be an indication for further surgery) and whether the mucosal resection margin is involved by carcinoma or the pre-existing adenoma (in which case a further local excision may be attempted).
There has been considerable discussion and controversy in the literature over what degree of clearance might be regarded as acceptable in tumours that extend close to the deep submucosal margin. It is important that this is measured and recorded in the report. It is likely that most would regard a clearance of <1mm as an indication for further therapy. Some would use <2mm and a few <5mm.
For an example of a polyp cancer:
Polyp cancer example
Comments
Comments/suggestions/feedback are welcome to patpq@leeds.ac.uk for consideration for the revision of these guidelines
REFERENCES
1. Konishi F, Morson MC. Pathology of colorectal adenomas: a colonoscopic survey. J Clin Pathol 1982; 35: 830-841.
2. Coverlizza S, Risio M, Ferrari A, Fenoglio-Preiser CM, Rossini FP. Colorectal adenomas containing invasive carcinoma: pathologic assessment of lymph node metastatic potential. Cancer 1989; 64: 1937-1947.
3. Cooper HS, Deppisch LM, Gourley WK et al. Endoscopically removed malignant colorectal polyps: clinicopathologic correlations. Gastroenterology 1995; 108: 1657-1665.
4. Volk EE, Goldblum JR, Petra RE, Carey WD, Fazio VW. Management and outcome of patients with invasive carcinoma arising in colorectal polyps. Gastroenterology 1995; 109: 1801-1807.
5. Haggitt RC, Glotzbach RE, Soffer EE, Wruble LD. Prognostic factors in colorectal carcinomas arising in adenomas: implications for lesions removed by endoscopic polypectomy. Gastroenterology 1985; 89: 328-36.
6. Kikuchi R, Takano M, Takagi K et al. Management of early invasive colorectal cancer. Risk of recurrence and clinical guidelines. Dis Colon Rectum 1995; 38: 1286-1295.
7. Nascimbeni R, Burgart LJ, Nivatvongs S, Larson DR. Risk of lymph node metastasis in T1 carcinoma of the colon and rectum. Dis Colon Rectum 2002; 45: 200-206.
8. Hamilton S R, Aaltonen L A 2000 Pathology and genetics of tumours of the digestive system. World Health Organization Classification of Tumors. Vol 2. IARC Press, Lyon
9. Makinen MJ. Colorectal Serrated adenocarcinoma. Histopathology 2007; 50: 131-15035. Halvorsen TB, Seim E. Degree of differentiation in colorectal adenocarcinomas: a multivariate analysis of the influence on survival. J Clin Pathol 1988; 41: 532-537.
10. Haboubi N, Geboes K, Shepherd N, Talbot I. Gastrointestinal Polyps. Greenwich Medical Media Limited: London; 2002: 95-123.
11. Jass JR, Williams CB, Bussey HJR, Morson BC. Juvenile polyposis: a pre-cancerous condition. Histopathology 1988; 13: 619-630
12. Muto T, Bussey HJR, Morson BC. Pseudocarcinomatous invasion in adenomatous polyps of the colon and rectum. J Clin Pathol 1973; 26: 25-31.
13. Ueno H, Mochizuki H, Hashiguchi Y, et al. Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology 2004; 127: 385-94.
APPENDIX A: TNM CLASSIFICATION OF COLORECTAL TUMOURS
pT Primary Tumour
pTX Primary tumour cannot be assessed
pT0 No evidence of primary tumour
pT1 Tumour invades submucosa
pT2 Tumour invades muscularis propria
pT3 Tumour invades through muscularis propria into subserosa or non-peritonealised pericolic or perirectal tissues
pT4 Tumour directly invades other organs (pT4a) and/or involves the visceral peritoneum (pT4b)
pN Regional Lymph Nodes
pNX Regional lymph nodes cannot be assessed
pN0 No regional lymph node metastasis
pN1 Metastasis in 1 to 3 regional lymph nodes
pN2 Metastasis in 4 or more regional lymph nodes
pM Distant Metastasis
pMX Distant metastasis cannot be assessed
pM0 No distant metastasis
pM1 Distant metastasis
APPENDIX B: SNOMED CODES COLORECTAL TUMOURS
T Codes
T-66000 Appendix
T-67000 Colon
T-68000 Rectum
M Codes
M-81400 Adenoma
M-74000 Dysplasia
M-80103 Carcinoma
M-81403 Adenocarcinoma
M-80703 Mucinous adenocarcinoma
M-84903 Signet ring cell adenocarcinoma
M-85603 Adenosquamous carcinoma
M-80703 Squamous cell carcinoma
M-80413 Small cell carcinoma
M-80203 Undifferentiated carcinoma
M-82433 Adenocarcinoid / goblet cell carcinoid tumour